
No Competence Needed
No Competence Needed
The Medical Practitioner's Tribunal delivers some dubious "facts"
Between July and October 2021, the Medical Practitioner’s tribunal sat to hear the case against Dr Helen Webberley, of GenderGP, and her competence to treat gender-questioning children. The determination of facts has now been published, and runs to 203 pages. It is, quite simply, a complete travesty.

It is hard to summarise without excerpting it at length, but, in brief:
The case focused on minors A, B and C, aged 12, 17 and 11 respectively at the time of treatment. In each case it was alleged that Webberley treated the children lacking competence in this area of medicine, and with inadequate psychological assessment beforehand or followup afterwards, giving puberty blockers and cross-sex hormones to children without establishing their capacity to consent or understanding of the likelihood that this would result in infertility. For example, in the case of C, the method of establishing that the child understood the treatment would render them infertile was to talk only to the mother, over the phone.
Many of those following the tribunal were appalled at the details that came out, but astonishingly this determination of facts dismisses pretty much all of these substantive charges, and while a few serious ones remain, many are trivial in comparison (such as inadequate record keeping, or whether blood pressure had been taken).
These determinations are reached on the following reasoning:
The question of whether Webberley is competent to deal with gender-questioning children is deemed irrelevant, because the tribunal believes there is a wider societal move to a more “enlightened” view that gender dysphoria should be “depathologised”. As such, it is not to be considered a mental health condition - or indeed a condition at all - and thus requires no real specialist knowledge.
The question of whether Webberley failed to provide adequate psychological assessment before rushing to prescribe puberty blockers and hormones fails for the same reason. If dysphoria is not a mental health condition, there is no need for such gatekeeping, which only stands in the way of the child’s self-actualisation - yet at the same time finds that expedited access to these interventions is warranted, or else the child may commit suicide.
The question of whether Webberley established that 11 and 12 year olds are competent to consent to irreversible medical interventions that lead to infertility and loss of sexual function is irrelevant because parents have an absolute right to consent on their behalf. Indeed, a child would need to be determined competent in order to refuse the parent’s wishes.
It is all based on a horrifying and contradictory chain of reasoning. Gender dysphoria is simultaneously not a mental health condition and something that needs urgent medicalisation on mental health grounds. A child’s self-knowledge is paramount and should be facilitated, medically, but simultaneously children lacking the capacity to consent to treatments they do not understand can have their self-knowledge overridden by their parent.
The tribunal is critical of NHS Gender Identity Development Service (GIDS) overly-tentative multidisciplinary approach, and praises WPATH’s continued push for early intervention, based on highly selective and superficial understanding of the evidence:

The cited evidence here is self-defeating, as all it does is indicate that children treated with blockers are likely to proceed to cross-sex hormones. This was one of the key points made during Bell v Tavistock, and one which this judgement completely fails to grasp. In other studies, children without such interventions are highly likely to desist over time (anything up to 90% of cases), and the majority grow up to be LGB adults.
It also makes some muddled claims around the onset of dysphoria, including the unsubstantiated (and highly contentious) statement that dysphoria manifesting during puberty is likely to persist.
On the subject of the Bell v Tavistock case, the tribunal says:
Here they misunderstand the nature of the “dispute”. The dispute was over whether the publicly stated purpose of blockers was truly to give children “time to think”, when in practice the actual purpose was cosmetic. That is, it was felt that if they blocked the development of secondary sex characteristics, the child could superficially “pass” as the opposite sex more easily once cross-sex hormones were administered.
But the tribunal takes all this as evidence that children don’t need “time to think”, because they have a stable “gender identity” quite young, and their self-knowledge should be facilitated. Indeed, the tribunal is critical of GIDS for acting as mental health gatekeepers, perpetuating the idea that gender dysphoria is a mental illness, and goes on to describe transgenderism as:
“a somatic (i.e. bodily; corporeal; physical) state of being, not a state of mind. This re-thinking is based on evidence that gender identity is innate, rather than learned”.
It then substantiates this highly contested claim with the following list of evidence:
John Money’s horribly unethical child abuse of the Reimar twins, in which a boy with a penis mutilated by a botched circumcision was experimentally raised as a girl, forced to simulate sex with his brother, and eventually killed himself.
Dubious connection between foetal exposure to androgens and later desire to transition that completely disregards all social and societal factors in between.
Adult transitioners’ revisionist anecdotes of lifelong feelings of dysphoria, which are notoriously unreliable since it is well understood that people will say what is required in order to gain access to transition, and in any case proves nothing about the stability or innateness of “gender identity”.
Complete garbage about post-mortem neurobiology pointing to structural causes of gender identity. Such studies have tiny sample sizes, riddled with false positives and all manner of confounding factors like neuroplasticity, age and sexuality, while modern brain imaging studies require many thousands of samples to show reliable correlations.
This whole thing is biological essentialism - that is, the idea that gendered behaviour and personality is the result an innate and natural “essence”. Women are deferential and compliant and wear dresses and makeup because that is the way women are innately supposed to be. A man who is deferential and compliant and wears dresses and makeup must do so because they are innately, biologically, structurally, a woman.
It is preposterous, regressive horseshit with the weakest possible foundation, several levels below the average poorly-thought out Facebook post, and harkens back to the “trans-as-intersex” beliefs of last century.
And it would be laughable if it wasn’t being used to justify sterilising gay children at their parents’ behest.
The tribunal decided that since gender dysphoria was being depathologised, it did not require any specialist knowledge to assess the best treatment:
The tribunal also decided that any co-presenting mental health conditions were the result of “minority stress”, and thus that affirmation and transition would resolve this distress. This being the case, it isn’t deemed necessary to seek any further mental health assessment to determine whether medical transition is appropriate, because they have reframed the distress at one’s sexed body not as a state of mind that needs consideration and treatment but as a state of being that should be affirmed. This reframing turns attempts to psychologically reconcile gender dysphoria into harm.

…

But later on they state - in order to justify Webberley’s rapid administering of hormone therapies with minimal consultation or waiting times - that “some patients with gender dysphoria are so desperate they are driven to suicide gives considerable impetus to this need for alternative approaches.”. Again: gender dysphoria is simultaneously not a mental health condition that needs specialist psychological assessment, but also a desperately life-threatening one that needs urgent treatment.
Several positive studies are cherry picked to show that paediatric transition is safe and effective, and at no point does the tribunal consider the weaknesses (ie the high dropout/lost-to-followup rate and lack of improvement in mental health) or the recent studies into regret and detransition.
Regarding consent, the tribunal - having previously decided that children’s self-knowledge is paramount - went on to declare that parents can consent for children who lack comprehension, so all questions as to Webberley having effectively established consent were moot. Not only that, if a child disagrees with the treatment, but is not Gillick competent, the parent can consent anyway:

I eagerly await condemnation of this determination from those who claim to be championing children’s right to bodily autonomy.
In the eyes of whoever wrote this document, 11-year olds know who they are, and should be medically facilitated in taking experimental treatment - primarily for cosmetic reasons - that will lead to infertility and loss of sexual function, irrespective of their ability to comprehend and consent, and suggesting that they may require psychological assessment beforehand is unenlightened, and all this should be done as quickly as possible before they kill themselves.
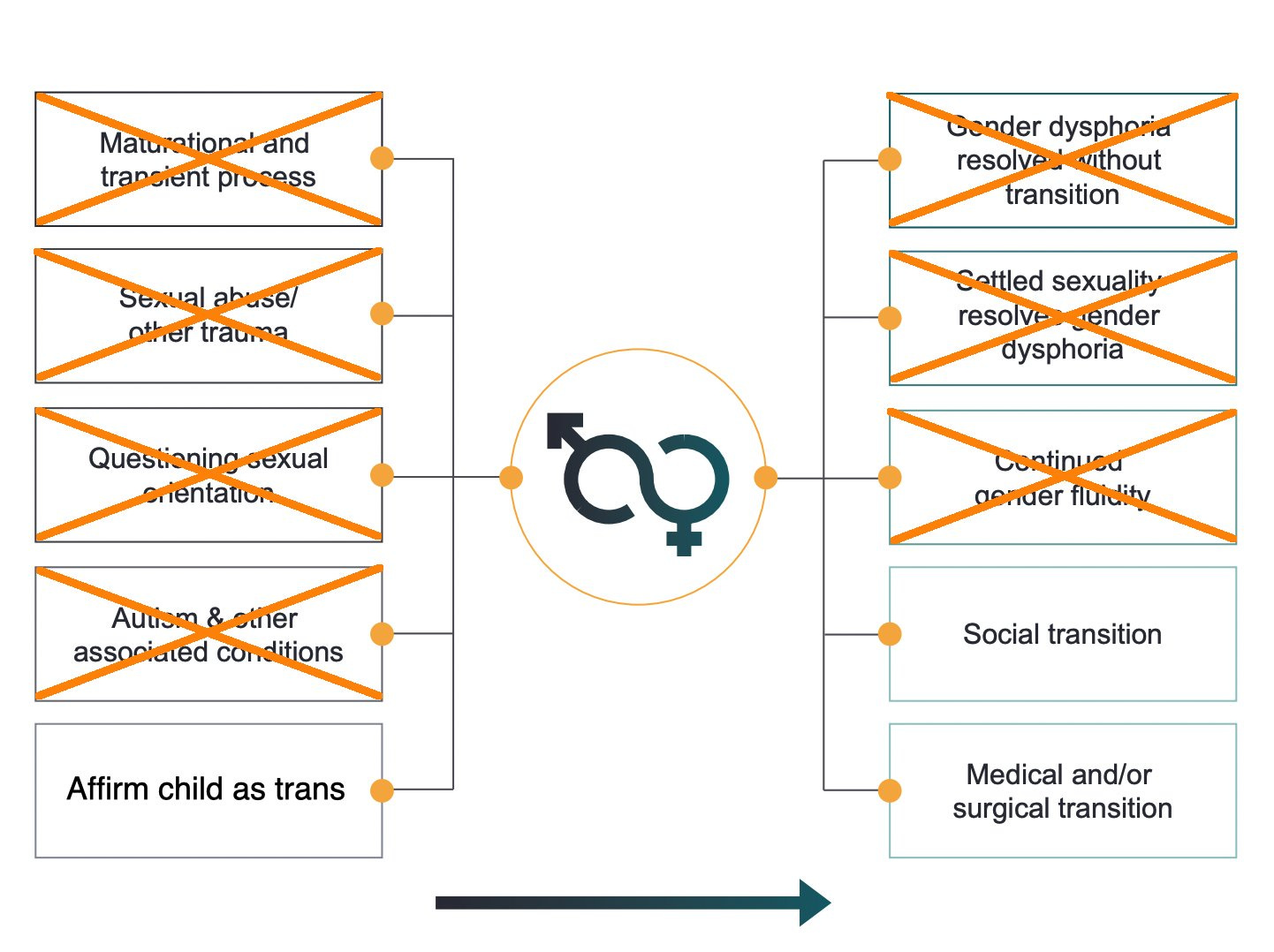
Compare this to the following diagram from the interim report of the Cass Review into gender treatment:
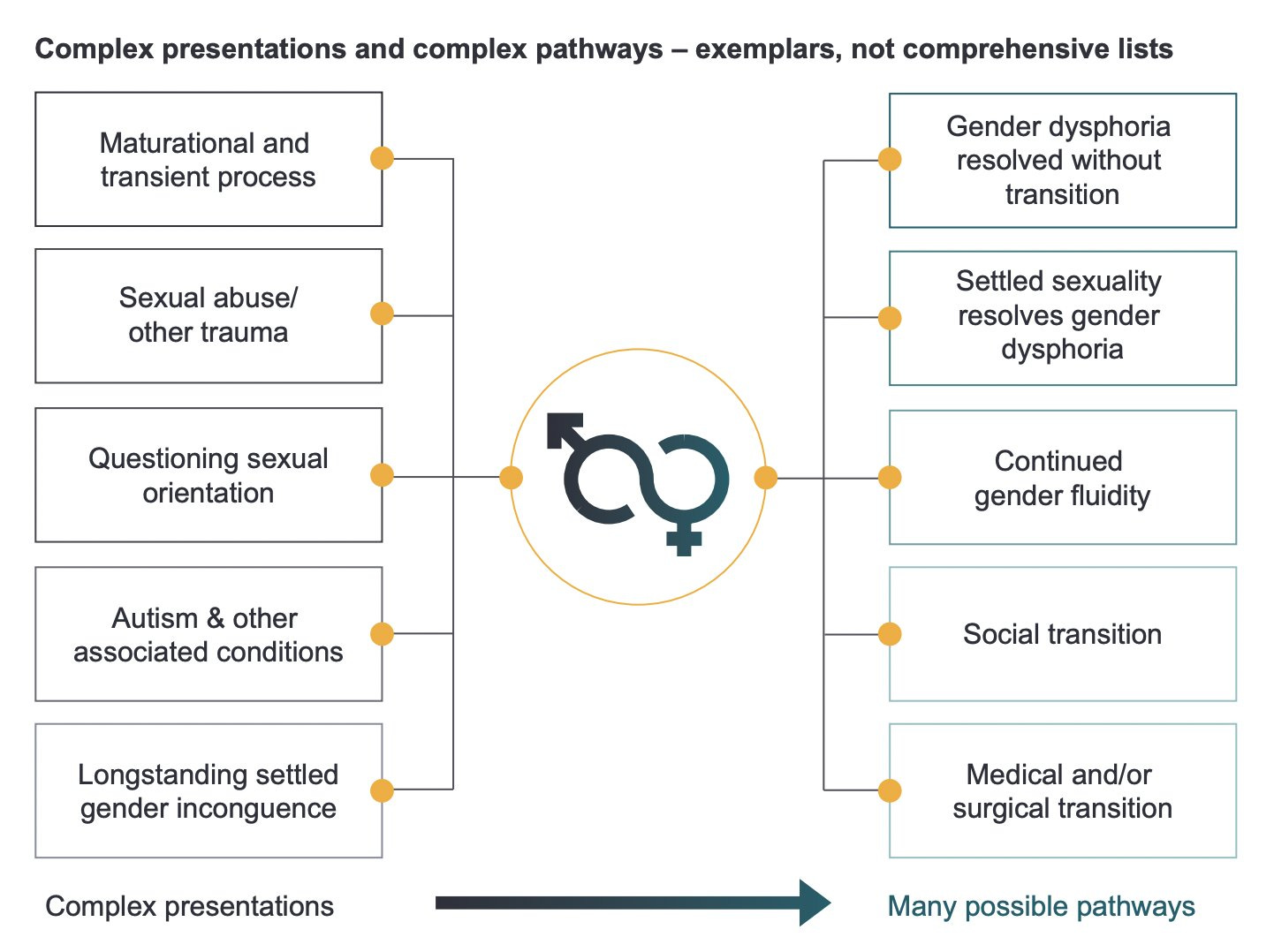
It is abundantly clear that feelings of distress in one’s own sexed body arise from many different causes, and have many different outcomes.
The view of the findings of fact against Helen Webberley collapses all of this into one possible - urgent - pathway, because children know who they are:
The belief that gender dysphoria should be “depathologised” completely prevents the consideration that it could ever be a symptom of other issues. It creates a moral imperative to never consider this possibility.
This is staggeringly irresponsible, and ignores all of the complex psychosocial factors that go into these feelings in favour of a quasi-religious belief that a child can have a wrong-sexed “essence” that requires their body be brought into accord, cosmetically, regardless of the consequence for later fertility or sexual function, and if necessary entirely on the say-so of the parent.
At around 7 minutes into this Emmy-winning documentary, we can see the homophobic response of the mother of Kai Shappley, who relentlessly beat her toddler son for wearing dresses and playing with dolls, until at age 4 he was praying to die:
“I remember even thinking before Kai was three that I think this kid might be gay. And I thought that that could not happen and that would not happen. We started praying fervently. Prayers turned into Googling "conversion therapy"and how can we implement these techniques at home to make Kai not be like this.”
All a boy this age will understand is that if girls play with dolls, and they themselves want to play with dolls, they must be a girl. If affirmed in this belief through social transition of course this child will be distressed once they hit adolescence and undeniable physical changes start to take place. Early social transition and affirmation exacerbates pubertal distress and makes desistance less likely, and medicalisation a near certainty.
This decision in the Webberley case would put all of the responsibility for these choices in the hands of parents, with doctors as wide-eyed facilitators of a child’s gender journey, with seemingly no accountability or oversight, on the grounds that it is more enlightened to do so, and that calling for psychological assessment and gatekeeping and the consideration of alternate pathways is just being a stick-in-the-mud who isn’t moving with the times.

This is start-to-finish an atrocious read, and at no point seems to seriously engage with or weigh up contrary evidence, or consider the rights of the child to be protected from unnecessary harm (well-meaning or otherwise), but simply swallows every rosy cherry-picked study and asinine talking point there is.